


INTRODUCTION
The incidence of olfactory disorders in the general populace ranges from 5% to 15%. These conditions not only significantly impact the quality of life of affected individuals, but also correlate with increased rates of morbidity and mortality [1-3]. The etiology of olfactory dysfunction is multifaceted, including factors such as post-viral and post-traumatic origins, allergic rhinitis, asthma, nasal obstruction, nasal surgery, xerostomia, neurodegenerative disorders, idiopathic causes, and notably, COVID-19 infection [4]. However, the rates of spontaneous recovery from these causes are limited, with only about one-third of patients experiencing a return of function, and this likelihood decreases with the length of the impairment [4,5]. Despite this, few treatment options exist for olfactory dysfunction. Empirical research highlights olfactory training and the use of topical or systemic corticosteroids as potential treatments, but their effectiveness is limited [3].
Encouragingly, the regenerative capacity of the olfactory neuroepithelium and olfactory filaments, as well as the peripheral nerve fibers extending through the cribriform plate into the nasal cavity, presents a plausible therapeutic target for individuals with olfactory dysfunction, including those who have experienced COVID-19-related loss of smell. Platelet-rich plasma (PRP), an autologous biological product derived from fresh whole blood characterized by a high platelet concentration, exhibits regenerative and anti-inflammatory properties, involving the upregulation of growth factors such as transforming growth factor, vascular endothelial growth factor, epidermal growth factor, and insulin-like growth factor [6]. PRP has been validated as a safe and effective treatment in various clinical scenarios, demonstrating efficacy in reducing inflammation, accelerating wound healing, stimulating nasal mucosa regeneration, and managing peripheral neuropathies [7-9]. Notably, PRP has shown the capacity to facilitate axon regeneration and neuroregeneration [10-13]. Therefore, we conducted a meta-analysis to assess the efficacy of PRP in treating persistent olfactory dysfunction, including cases associated with COVID-19 infection.
METHODS
This investigation adhered to the guidelines outlined in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA). The requirement for Institutional Review Board (IRB) approval was waived for this study, given its nature as a systematic review and meta-analysis reliant solely upon published literature.
The population, intervention, comparison, and outcomes (PICO) criteria for this study were as follows: population— patients with chronic olfactory dysfunction lasting more than 6 months refractory to current known treatments (olfactory training, steroid administration, etc.); intervention—topical administration of PRP; comparison—not limited; and outcomes—changes in olfactory scoring systems including the Sniffin’ Sticks test (threshold, discrimination, and identification [TDI] score), Connecticut Chemosensory Clinical Research Center (CCCRC) olfaction test, Q-Sticks test, visual analogue scale (VAS), or significant improvement of olfactory dysfunctions. This review adhered to the recommendations of the PRISMA guideline [14].
Studies were searched on PubMed, Scopus, Embase, the Web of Science, Google Scholar, and the Cochrane database. All prospective articles published before January 2024 were retrieved. Key search terms included anosmia, hyposmia, olfactory, smell, olfactory disorders, olfactory dysfunctions, recovery, olfactory test, platelet-rich plasma, olfactory cleft, olfactory fissure, nasal mucosa, injection, and treatment. Two independent literature reviewers meticulously assessed and screened the titles and abstracts of all identified studies, excluding those unrelated to the subject matter. If the abstract alone did not provide sufficient information for inclusion determination, the full text was comprehensively evaluated. Discrepancies in document selection between the two reviewers were resolved through deliberation with a third reviewer. Efforts were undertaken to solicit additional details directly from authors in instances of missing or incomplete data.
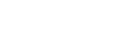
The exclusion criteria involved studies on olfactory dysfunction arising from obstructive or inflammatory lesions, as well as those with multiple reports based on the same trial data. Studies lacking clear and quantifiable data reporting or where appropriate data extraction and calculation were not feasible from the published results were also excluded from the analysis. A visual representation of the study selection process is presented in Fig. 1.
Data extraction and risk of bias assessment
Data were systematically extracted from the selected eligible studies using a standardized format [15,16]. Information regarding patient number, the grading scale employed for assessing olfactory dysfunction, the incidence or percentage of individuals exhibiting substantial recovery from olfactory dysfunction, and the p-value for the comparison between the treatment and control groups or between pre-treatment and post-treatment outcomes was extracted [17-26]. The analyzed outcomes included changes in olfactory scores after treatment and the percentage of individuals who significantly recovered from olfactory dysfunction. These results were compared between the treatment group (topically administered PRP) and the control group (saline or no treatment), as well as between pre- and post-treatment. Risk of bias assessment in randomized controlled studies was conducted utilizing the Cochrane risk of bias tool (as presented in Supplementary Table 1 in the online-only Data Supplement) [12], while non-randomized controlled studies were appraised using the Newcastle-Ottawa Scale (with scores ranging from 0 to 9, as delineated in Supplementary Table 2 in the online-only Data Supplement).
Statistical analysis
Meta-analyses of the identified studies were undertaken using the R statistical software version 4.3.2 (R Foundation for Statistical Computing, Vienna, Austria). In instances where original data were presented as continuous variables, the meta-analysis utilized either standard mean differences (SMD) or mean differences to calculate the effect size, due to the absence of standardized metrics for the assessment of olfactory functions (such as self-olfactory scoring, VAS, and the Sniffin’ Sticks test). For all other cases, the incidence of outcomes was analyzed using odds ratios (ORs). Sensitivity analyses were conducted to gauge the impact of each individual study on the overall results of the meta-analysis.
RESULTS
Degree of change in olfactory scores between the treatment group and control group
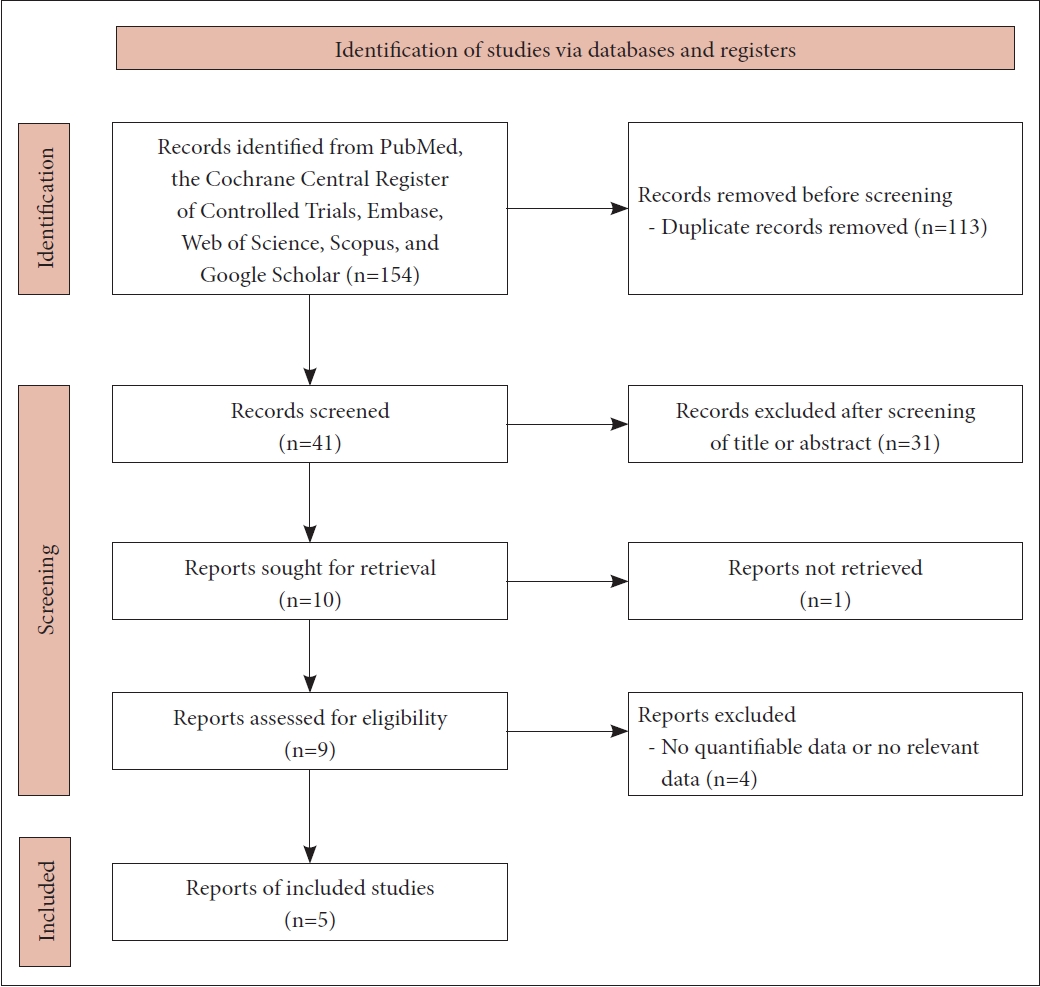
The treatment group exhibited a significantly greater improvement in olfactory scores at post-treatment intervals of 1 to 3 months compared to the control group (SMD=1.4376; 95% confidence interval [CI]=0.5934–2.2818; I2=84.1%). Notably, a considerable degree of inter-study heterogeneity (I2> 50) was observed in the results. Two different types of olfactory assessment, subjective (self-olfactory scoring or VAS) and objective tests (validated olfactory psychophysical tests such as the Sniffin’ Sticks test, CCCRC olfaction test, or Q-Sticks test), were utilized. The effects of PRP might vary depending on the olfactory assessment. Therefore, a subgroup analysis was undertaken to evaluate the variance in the comparative advantage of topical PRP in terms of the type of olfactory assessment. The analysis revealed no statistically significant differences in the improvement of olfactory scores at the post-treatment period of 1 to 3 months (SMD=1.7763; 95% CI=0.2873–3.2654 vs. SMD=1.1492; 95% CI=-0.0863 to 2.3848; p=0.5253) between the objective subgroup and the subjective subgroup. These findings could indicate that the treatment would have a beneficial effect on olfactory function regardless of the type of olfactory test used (Fig. 2A).
Percentage of significant recovery from olfactory dysfunction between the treatment group and control group
A substantial difference was observed in the incidence of significant recovery from olfactory dysfunction between the treatment group and the control group (OR=8.6639; 95% CI=2.9752–25.2292; I2=0.0%). Furthermore, within the subgroup analysis, no statistically significant differences were identified in the incidence of substantial recovery from anosmia between the objective subgroup and the subjective subgroup (OR=14.6667; 95% CI=1.4637–146.9601 vs. OR=7.5000; 95% CI=2.2445–25.0616; p=0.6133). These findings suggest that PRP treatment could have a beneficial effect on olfactory function regardless of the type of olfactory test used (Fig. 2B).
Changes in olfactory measurements after platelet-rich plasma treatment
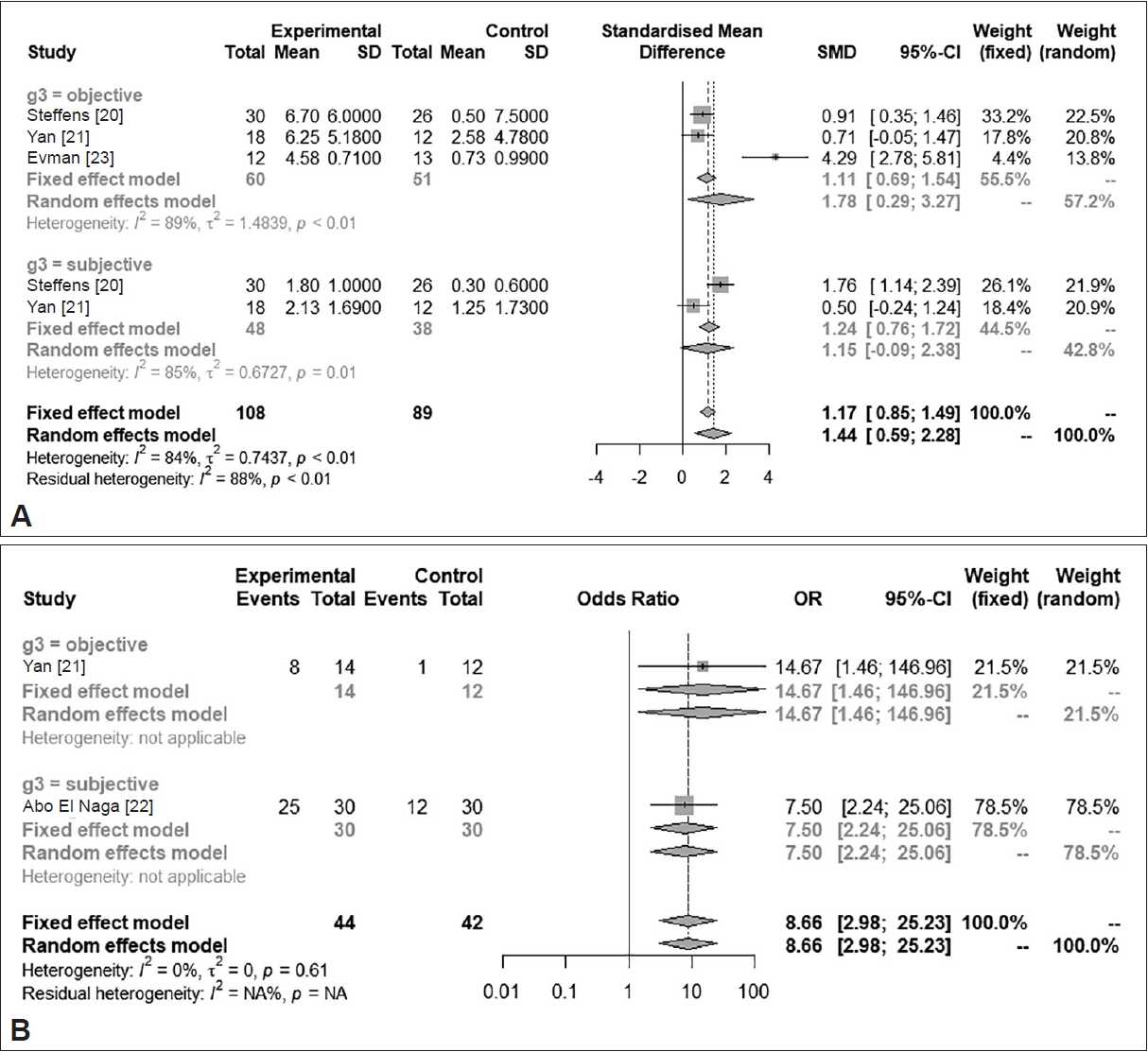
The OR for significant improvement after treatment was 0.7654 (95% CI=0.6612–0.8451; I 2 =0.0%) (Fig. 3A). The included studies utilized subjective (self-olfactory scoring or VAS) and objective tools (validated olfactory psychophysical tests, such as the Sniffin’ Sticks test, CCCRC olfaction test, and Q-Sticks test) for determining significant improvement in olfactory function. In the subgroup analysis according to the type of olfactory assessment, statistically significant differences were found in the likelihood of significant improvement between the objective and subjective subgroups (OR=0.5714; 95% CI=0.3163–0.7935 vs. OR=0.8060; 95% CI=0.6939–0.8839; p=0.0678). These findings suggest that patients may be satisfied with the treatment psychologically, as well as achieving favorable results in terms of validated olfactory outcomes. PRP treatment led to an increase of more than 5.5 (the minimal clinically important difference) in the TDI score of the Sniffin’ Sticks test (mean difference=6.3494; 95% CI=4.0605–8.6384; I 2 =0.0%), which could be considered a clinically significant improvement based on verified examinations (Fig. 3B). All subdomains in the olfactory function test (threshold, discrimination, and identification) significantly and similarly improved after treatment (threshold SMD=0.8694; 95% CI=0.0513–1.6876; discrimination SMD=0.6345; 95% CI=0.1669–1.1022; identification SMD=2.2560; 95% CI=-1.3115–5.8235; p=0.6166) (Fig. 3C).
DISCUSSION
This study confirms that local administration of PRP accelerates the improvement of olfactory function and leads to significant improvement in olfactory scores compared to the control group for patients with persistent and refractory olfactory disorders. The observed improvement in olfactory function signifies a clinically significant recovery across all categories: threshold, discrimination, and identification. It is particularly noteworthy that the studies included in this analysis predominantly targeted patients with persistent olfactory dysfunction lasting more than 6 months. PRP treatment proved effective across all sensory-neuronal types and also in patients with a reduced sense of smell after COVID-19 infection.
Proven medical treatments for improving olfactory dysfunction are limited. While corticosteroids are commonly used in clinical practice, their precise mechanism of action remains poorly understood. According to the prevailing hypothesis, the anti-inflammatory properties inherent to corticosteroids contribute to their therapeutic effects [3]. The use of alternative interventions such as ginkgo biloba, zinc, retinoic acid, α-lipoic acid, caroverine, minocycline, and phosphodiesterase inhibitors (e.g., theophylline) has been reported. However, evidence supporting the efficacy of these alternative treatments is lacking [2]. Hence, there continues to be an unmet need for treating olfactory disorders, particularly those unrelated to sinonasal inflammation.
Reports indicate that PRP is effective in promoting the regeneration of the tympanic membrane, vocal folds, and facial nerves, as well as in addressing atrophic rhinitis [27]. Additionally, PRP has shown promise in improving the healing process following tympanoplasty or endoscopic sinus surgery [8,27]. Furthermore, PRP’s autologous nature mitigates the risk of allergic or immune rejection reactions, and its rapid preparation involves a straightforward process with two centrifugation stages.
PRP, an autologous biological product derived from fresh whole blood with a high concentration of platelets, has demonstrated effectiveness and safety in treating persistent olfactory dysfunction associated with COVID-19. Due to its autologous origin, the likelihood of rejection or adverse reactions is exceedingly rare. While only a limited number of studies have explored the efficacy of PRP in human subjects, both case-control studies and non-controlled clinical trials have indicated its effectiveness. PRP may facilitate peripheral nerve regeneration by promoting vascular and axonal growth through growth factors and by modulating inflammatory responses within the microenvironment, which could explain the observed beneficial effects.
While the results of this meta-analysis offer promising implications for treating patients with olfactory dysfunction, several limitations exist. First, the dose and frequency of PRP administration varied across studies, without standardization. Additionally, there is a lack of standardized or optimal recommendations regarding PRP injection dosage or concentration. Second, the inclusion of various etiologies in the meta-analysis may have resulted in heterogeneity. Third, while validated psychophysiological tests for olfaction were prioritized, subjective improvements (VAS or the proportion of patients with significant improvement) were not excluded from the outcomes. Future studies should prioritize establishing validated psychophysiological tests as primary outcomes to generate objective results. Current reports include case series and single-arm studies, and well-designed studies involving large patient populations are still lacking. Given the high prevalence of hyposmia and the continuing emergence of positive reports about PRP, further interest and follow-up research are warranted.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Supplement1
Supplement1 Print
Print






